A meta-analysis of cigarette smoking, bone mineral density and risk of hip fracture: recognition of a major effect
BMJ 1997; 315 doi: https://doi.org/10.1136/bmj.315.7112.841 (Published 04 October 1997) Cite this as: BMJ 1997;315:841
- a Department of Environmental and Preventive Medicine, Wolfson Institute of Preventive Medicine, St Bartholomew's and The Royal London School of Medicine, London EC1M 6BQ
- Correspondence to: Dr Law
- Accepted 3 June 1997
Abstract
Objective: To determine the magnitude and importance of the relation between smoking, bone mineral density, and risk of hip fracture according to age.
Design: Meta-analysis of 29 published cross sectional studies reporting the difference in bone density in 2156 smokers and 9705 non-smokers according to age, and of 19 cohort and case-control studies recording 3889 hip fractures reporting risk in smokers relative to non-smokers.
Results: In premenopausal women bone density was similar in smokers and non-smokers. Postmenopausal bone loss was greater in current smokers than non-smokers, bone density diminishing by about an additional 2% for every 10 year increase in age, with a difference of 6% at age 80. In current smokers relative to non-smokers the risk of hip fracture was similar at age 50 but greater thereafter by an estimated 17% at age 60, 41% at 70, 71% at 80, and 108% at 90. These estimates of relative risk by age, derived directly from a regression analysis of the studies of smoking and hip fracture, were close to estimates using the difference in bone density between smokers and non-smokers and the association between bone density and risk of hip fracture. The estimated cumulative risk of hip fracture in women in England was 19% in smokers and 12% in non-smokers to age 85; 37% and 22% to age 90. Among all women, one hip fracture in eight is attributable to smoking. Limited data in men suggest a similar proportionate effect of smoking as in women. The association was not explained by smokers being thinner, younger at menopause, and exercising less nor by actions of smoking on oestrogen, but smoking may have a direct action on bone.
Conclusions: Hip fracture in old age is a major adverse effect of smoking after the menopause. The cumulative excess bone loss over decades is substantial, increasing the lifetime risk of hip fracture by about half
Key messages
Smoking has no material effect on bone density in premenopausal women
Postmenopausal bone loss is greater in smokers—an additional 0.2% of bone mass each year. The cumulative effect of this over many years is substantial, with a difference of 6% at age 80
In current smokers relative to non-smokers the risk of hip fracture is estimated to be 17% greater at age 60, 41% greater at 70, 71% greater at 80, 108% greater at 90
The data in men are limited but suggest a similar proportionate effect in smokers
The cumulative risk of hip fracture to age 85 in women is 19% in smokers and 12% in non-smokers; to age 90 it is 37% and 22%
Among all women, one hip fracture in eight is attributable to smoking
Introduction
A lower bone mineral density in smokers was shown 20 years ago,1 but the importance of the relation, and its association with age, remained uncertain despite the large number of published studies.1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 There have been conflicting conclusions from individual studies—that smoking is an unimportant determinant of low bone density and fracture risk,27 that it has only an indirect effect on bone density (by reducing age at menopause or body weight),15 24 that it is important only in women receiving hormone replacement therapy (as it reduces the protective effect),13 34 and that it is an important direct cause of bone loss.23 30 It has been concluded from individual studies both that among young adults bone density is lower in smokers3 5 14 and that it is not,2 6 and that postmenopausal bone loss is greater in smokers18 and that it is not.14 17 51 We seek to resolve the uncertainty by an analysis of published data on smoking, bone mineral density, and hip fracture according to age.
Methods
We identified published studies measuring bone mineral density (by absorptiometry or computed tomography) or recording the incidence of hip fracture in women according to their smoking habit, using Medline (MeSH terms and textwords “smoking or tobacco” “bone density or osteoporosis or hip fracture”). We also examined the reference lists of the studies and of review articles. We excluded studies in which the subjects were selected because they had some disease, such as diabetes, and one case-control study in which any effect of smoking was likely to be small because the smokers did not start smoking until age 58 on average (the study was conducted in countries in which women took up smoking only recently).52 All other studies were included.
In studies of bone density, separate data were available on premenopausal and postmenopausal women (defining postmenopausal as the absence of cyclical bleeding usually for six months, sometimes less), except in five studies of perimenopausal women in which all women had to be assigned to the category (premenopausal or postmenopausal) that included the majority. Unpublished data were obtained from the authors of one study which recruited premenopausal and postmenopausal women over a wide age range (27-73 years).10 We recorded bone density measurements in the femoral neck, radius, or calcaneus (in that order of preference if measurements at more than one site were reported). The difference between the average bone density of current smokers and non-smokers in each study was recorded as a proportion of one standard deviation (SD) since absolute bone density units varied between studies according to the bone and the measurement technique. We ensured that the difference in bone density was adjusted for age when the mean age of smokers and non-smokers was not the same, but we did not include data adjusted for body weight or other determinants of bone density in the analysis except in three studies that reported only the adjusted results.23 28 30 We conducted linear regression analyses of the difference in bone density between current smokers and non-smokers in each study, separately in premenopausal and postmenopausal women, on the mean age of the women. Each bone density difference was weighted by the inverse of its variance (the sum of the inverse of the numbers of smokers and non-smokers).
The cohort and case-control studies of the incidence of hip fracture in smokers relative to non-smokers excluded hip fractures caused by high energy trauma (fall from a height, road traffic accident) and fractures in metastatic bone. All the women with fractures were postmenopausal except in two studies in which a minority were premenopausal.31 32 In five studies a total of 23% of the subjects were men and sex specific data were not published, but 94% of all the subjects in the 19 studies were women. We determined the mean age at fracture in each study; where this could not be calculated from published data it was provided by the authors.37 38 46 49 We ensured that the relative risk estimates were adjusted for age, but again did not include estimates adjusted for body weight or other determinants of fracture in the analysis except in four studies where only this was reported.33 41 44 45 We conducted a linear regression analysis of the risk of hip fracture in smokers relative to non-smokers in each study (weighted by the inverse of its variance) on the mean age at the time of the fracture. The resulting direct estimates of the risk of fracture in smokers relative to non-smokers according to age were compared with indirect estimates derived using the differences in bone density in SDs (calculated above) and the relative risk of hip fracture for a decrease of 1 SD in femoral neck bone density (taken as 2.7, the pooled estimate from two cohort studies53 54 and an analysis of 10 case-control studies55).
Estimates of the age specific incidence of hip fracture were derived separately for current smokers and never smokers, using the age specific rates of hospital admission for hip fracture among all women in England in 1992-3.56 This was done by apportioning the fractures in each 10 year age group to current smokers, never smokers, and former smokers in 10 year categories of time since stopping smoking, using survey data on the prevalence by age of current and former smokers among women in England57 and the age specific relative risk in current smokers (the direct estimates calculated above) and in former smokers (taken as the relative risk corresponding to the age at which they stopped smoking). In each 10 year age group we then calculated the attributable proportion—that is, the number of hip fractures in women attributable to smoking (the difference between the total number of fractures and the number expected in the population from the incidence in never smokers) divided by the total number of fractures.
Results
Table 1 shows details of the 29 cross sectional studies of bone density according to smoking habit and age. The average bone density was reported in current smokers alone in all the studies, and in never smokers alone in most studies (including all studies in women aged 65 and over) but only in former smokers and never smokers combined in some studies (mainly those of younger women). In all the studies there were 2156 smokers and 9705 non-smokers.
Cross sectional studies of bone density according to smoking status in women
Figure 1 shows the age adjusted differences in bone mineral density between smoking and non-smoking women according to the mean age and menopausal status in these studies. The linear regression lines fit the data well. In premenopausal women the confidence intervals excluded any material association between smoking and bone density. The estimated difference in bone density between smokers and non-smokers irrespective of age was 0.01 SD (95% confidence interval −0.10 to 0.11 SD) or about 0.1% (−1% to 1%) of the average bone density. The estimated difference per 10 year age increase was 0.04 SD (−0.06 to 0.14 SD). In postmenopausal women bone density was lower in smokers than non-smokers, and the difference increased linearly with age (P=0.001). For every 10 year increase in age the bone density of smokers fell below that of non-smokers by 0.14 SD (0.07 to 0.21 SD), equivalent to about 2% (1% to 3%) of the average bone density at the time of the menopause. The estimates of the association were virtually identical in three separate analyses of the studies measuring bone density in the femoral neck, radius, and calcaneus.
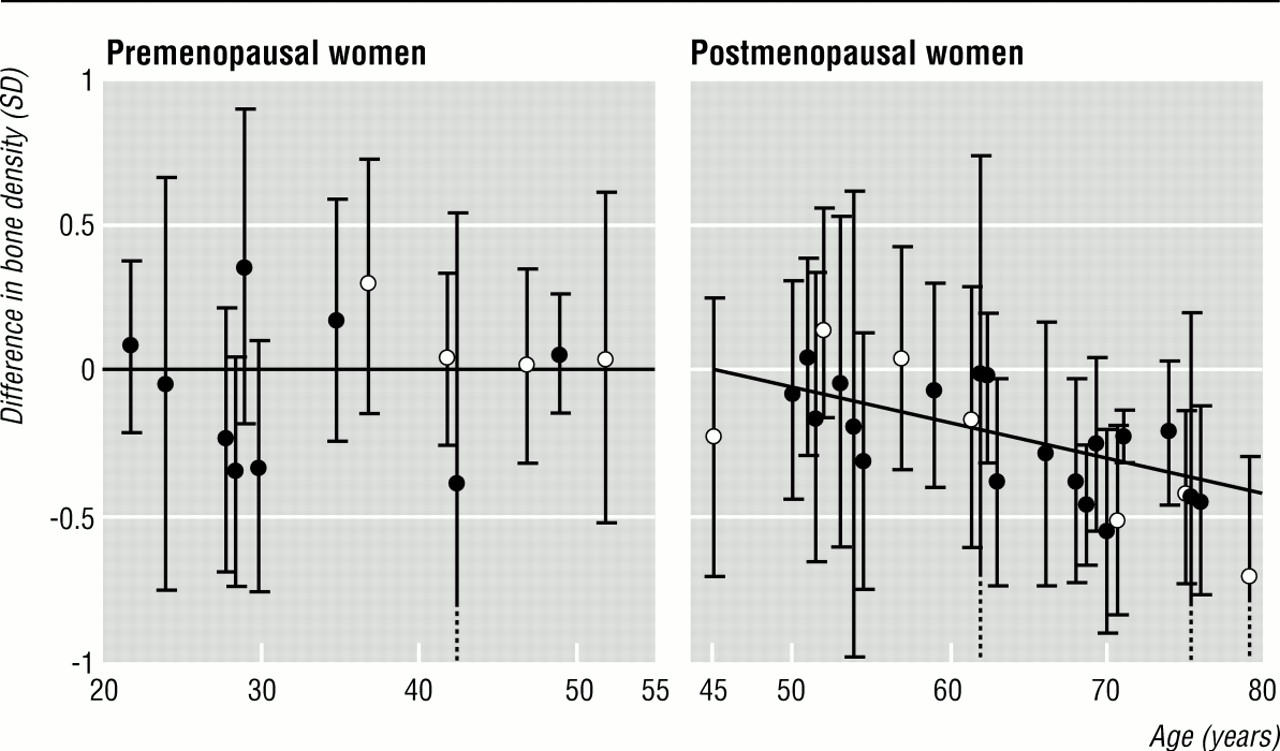
Differences (95% confidence intervals), as a proportion of 1 SD, in bone mineral density between female smokers and non-smokers according to age and menopausal status. Fitted regression lines are shown. The 11 open circles refer to two studies Figure 9 26solid circles refer to the other studies in the order listed in Table 1
{kind=link}
Table 2 shows details of the 19 cohort and case-control studies of the risk of hip fracture in postmenopausal women according to smoking habit and age. In total there were 3889 hip fractures. Variation between the studies in the average age at fracture arose because of differences in the upper age limit of women recruited and, in cohort studies, in duration of follow up. Estimates of risk in current smokers relative to that in never smokers were reported in 10 studies but were available only with former smokers included with current smokers in four studies and with never smokers in five. Figure 2 shows the risk of hip fracture in smokers relative to that in non-smokers according to age in the 19 studies. Relative risk increased significantly with age (P<0.001), and the log linear regression line fitted the data well (59% of the variation was accounted for).
Cohort and case-control studies of risk of hip fracture in female smokers relative to female non-smokers

Relative risk (95% confidence intervals) of hip fracture in smokers compared with non-smokers in postmenopausal women according to age, in cohort studies (solid circles) and case-control studies (open circles), each in the same order as in table 2. Fitted regression line is shown
{kind=link}
Table 3 shows estimates of the effect of smoking on bone density in postmenopausal women according to age, from the regression line in figure 1. By the age of 80, bone density was 0.45 SD (6%) lower in smokers than non-smokers. Table 3 also shows the risk of hip fracture in smokers relative to non-smokers according to age as predicted from the differences in bone density (from the relation between femoral neck bone density and risk of hip fracture), and as estimated directly from the regression line in figure 2. These indirect estimates are remarkably close to the direct estimates of the relative risk of hip fracture at different ages. Smoking has no effect on risk at age 50 but (using the direct estimates) risk of hip fracture is 17% greater in smokers than non-smokers at the age of 60, 41% greater at age 70, 71% greater at age 80, and 108% greater at age 90.
Estimates (95% confidence intervals) of effect of smoking on bone density and risk of hip fracture in postmenopausal women according to age
Table 4 shows the cumulative incidence of hip fracture according to age in women who currently smoke and women who never smoked. An estimated 19% of current smokers and 12% of never smokers would have a hip fracture by the age of 85, 37% and 22% respectively by the age of 90. Table 4 also shows estimates by age of the proportion of all hip fractures attributable to smoking (that is, the excess incidence in current and former smokers as a proportion of the incidence among all women). Over all ages, 13% of all hip fractures in women are attributable to smoking.
Estimated incidence of hip fracture in smokers and non-smokers among women, England, 1992-3
The relation between smoking and low bone density was largely independent of the lower average body weight of smokers (bone density is lower in thin people) and of associations of smoking with other factors that reduce bone density such as lack of exercise.21 26 27 29 In the largest study, for example, the estimated difference between smokers and non-smokers was 0.25 SD before and 0.18 SD after adjustment (P<0.001).27 The effect of oestrogen replacement therapy could be ignored since only a minority of the women in the studies had used it at all, and generally for a year or less; the most prevalent usage in all the studies was 18% of the women taking therapy for 2 years or more.19 The relation between smoking and hip fracture was also not materially changed after adjustment for body mass index, exercise, and oestrogen use. This could be assessed in 10 studies in which the estimated relative risks with and without such adjustment were reported. The combined estimate was 1.54 (1.32 to 1.80) adjusted only for age and 1.46 (1.28 to 1.64) adjusted also for other factors; the difference was not significant.
In women who smoked, the average daily cigarette consumption was about 15.5 6 12 13 16 20 There was a dose-response relation between risk of hip fracture and number of cigarettes smoked.34 39 43 45 46 47 50 In former smokers the effect on both bone density23 25 26 30 and risk of fracture35 37 45 50 was intermediate between that in never smokers and current smokers.
In men the number of studies is too low and the variation in mean age between studies is too narrow to permit a regression analysis on age similar to that conducted in women. There are, however, five published studies comparing femoral neck bone density between smokers and non-smokers in men aged 65-77,21 23 28 30 58 and the combined estimate of the difference in bone density was 0.32 SD (0.19 to 0.45 SD) lower in smokers, applicable to a mean age of 71. This is remarkably similar to the estimate for women in the same age group (Table 3). The two studies that recorded reasonable numbers of fractures in older men as well as women suggest a similar effect of smoking on the risk of hip fracture in the two sexes.36 37 The proportionate effect of smoking is therefore likely to be similar in men and women.
Discussion
Smoking is a major cause of hip fracture. It increases the lifetime risk by about half, from an estimated 12% to 19% in women up to the age of 85, and from 22% to 37% to the age of 90. Of all hip fractures, one in eight is attributable to smoking.
The effect of smoking on bone mineral density increases cumulatively with age. There is no detectable effect in premenopausal women. Postmenopausal bone loss is greater in smokers, but the excess, while statistically significant, is small—0.2% of the average bone density at the menopause per year. It is not surprising, therefore, that studies measuring the rate of bone loss in the same women a few years apart14 20 51 and cross sectional studies of women a few years after the menopause12 13 14 15 16 17 18 19 have found little or no effect of smoking. It is the cumulative excess postmenopausal bone loss over many years that makes smoking an important cause of fracture. By the age of 80, when hip fracture is a major health problem, the accumulated additional loss of bone in smokers of 6% translates into an estimated 71% greater risk of hip fracture.
The association of smoking with low bone density and hip fracture is undoubtedly cause and effect. Risk was lower in former smokers, and in current smokers there was a dose-response relation with the number of cigarettes smoked. Adjustment for potential confounding factors had little effect. Different types of study produced similar estimates: the estimate of the excess risk of hip fracture in smokers from the analysis of the studies of smoking and hip fracture was remarkably close to that from the studies of smoking and bone density (given the association between bone density and hip fracture). The effect of current smoking on both bone density and risk of hip fracture will be underestimated a little because some studies included former smokers with either current or never smokers.
Mechanisms
Various mechanisms whereby smoking increases postmenopausal bone loss can be postulated, but their importance is uncertain. There may be a direct toxic effect on bone; animal data show that formation of new bone is impaired on exposure to nicotine.59 Smoking may reduce calcium absorption.18 Cortisol, which lowers bone density, is raised transiently after smoking,60 but it is similar cross sectionally in smokers and non-smokers9 61 and any effect on bone density must be small, or else a lower bone density would have been observed in premenopausal smokers. Lastly, the risk of falling in elderly people is a little greater in smokers,62 63 and this is consistent with the suggestion in Table 3 that the risk of hip fracture in smokers may be slightly greater than expected from their lower bone density.
The more commonly postulated mechanisms account for little of the effect on bone density. The lower average body weight of smokers was relatively unimportant. Actions of smoking on oestrogen are not likely to explain the lower bone density of smokers. In premenopausal women, smoking has little or no effect on bone density irrespective of its effect on oestrogens, while postmenopausal smokers lose bone faster but their plasma concentrations of endogenous oestrogen are no lower than those of non-smokers.9 60 64 Among women receiving oral oestrogen replacement, oestrogen is lower in smokers because of increased hepatic metabolism,12 13 but in almost all the studies reviewed only a small fraction of the women took oestrogen replacement for more than a year. The earlier menopause in smokers (earlier by about 1.5 years60) advances the period of postmenopausal rapid bone loss, but this makes little difference in old age: smokers at the age of 80 (about the mean age of hip fractures) would have the same average bone density as non-smokers aged 81.5 years (a difference of about 0.04 SD65 compared with the overall difference of 0.45 SD). Furthermore, the similar effect of smoking on bone density and risk of fracture in men as in women is against the effect being mediated through lower oestrogen concentrations or age of menopause.
Conclusion
Smoking in women from the time of the menopause onwards increases the risk of hip fracture in old age by about half. This is an insufficiently recognised major adverse effect of smoking, and it has substantial implications on healthcare costs. The lower risk in former smokers indicates that stopping smoking prevents further excess bone loss, and stopping at the time of the menopause should avoid the excess risk.
Acknowledgments
We thank the following investigators for unpublished data from the referenced studies: J Hopper and E Seeman,10 A Paganini-Hill,37 46 and C Wickham.38 39
Source of Funding: None.
Conflict of interest: None.