Interventions to reduce unintended pregnancies among adolescents: systematic review of randomised controlled trials
BMJ 2002; 324 doi: https://doi.org/10.1136/bmj.324.7351.1426 (Published 15 June 2002) Cite this as: BMJ 2002;324:1426
- Alba DiCenso (dicensoa{at}mcmaster.ca), professora,
- Gordon Guyatt, professorb,
- A Willan, professorc,
- L Griffith, data analystd
- a School of Nursing, McMaster University, 1200 Main Street West, Hamilton, Ontario, Canada L8N 3Z5
- b Departments of Clinical Epidemiology and Biostatistics, McMaster University, 1200 Main Street West, Hamilton, Ontario
- c Department of Clinical Epidemiology and Biostatistics, McMaster University, 105 Main Street East, Level P1, Hamilton, Ontario, Canada L8N 1G6
- d Department of Clinical Epidemiology and Biostatistics, McMaster University, 1200 Main Street West, Hamilton, Ontario
- Correspondence to: A DiCenso
- Accepted 7 February 2002
Abstract
Objective: To review the effectiveness of primary prevention strategies aimed at delaying sexual intercourse, improving use of birth control, and reducing incidence of unintended pregnancy in adolescents.
Data sources: 12 electronic bibliographic databases, 10 key journals, citations of relevant articles, and contact with authors.
Study selection: 26 trials described in 22 published and unpublished reports that randomised adolescents to an intervention or a control group (alternate intervention or nothing).
Data extraction: Two independent reviewers assessed methodological quality and abstracted data.
Data synthesis: The interventions did not delay initiation of sexual intercourse in young women (pooled odds ratio 1.12; 95% confidence interval 0.96 to 1.30) or young men (0.99; 0.84 to 1.16); did not improve use of birth control by young women at every intercourse (0.95; 0.69 to 1.30) or at last intercourse (1.05; 0.50 to 2.19) or by young men at every intercourse (0.90; 0.70 to 1.16) or at last intercourse (1.25; 0.99 to 1.59); and did not reduce pregnancy rates in young women (1.04; 0.78 to 1.40). Four abstinence programmes and one school based sex education programme were associated with an increase in number of pregnancies among partners of young male participants (1.54; 1.03 to 2.29). There were significantly fewer pregnancies in young women who received a multifaceted programme (0.41; 0.20 to 0.83), though baseline differences in this study favoured the intervention.
Conclusions: Primary prevention strategies evaluated to date do not delay the initiation of sexual intercourse, improve use of birth control among young men and women, or reduce the number of pregnancies in young women.
What is already known on this topic
Unintended pregnancies among adolescents pose a considerable problem for the young parents, the child, and society
What this study adds
Primary prevention strategies evaluated to date do not delay the initiation of sexual intercourse or improve use of birth control among adolescents
Primary prevention strategies have not reduced the rate of pregnancies in adolescent women
Meta-analysis of five studies, four of which evaluated abstinence programmes, has shown an increase in pregnancies in partners of male participants
Introduction
The period between childhood and adulthood is a time of profound biological, social, and psychological changes accompanied by increased interest in sex. This interest places young people at risk of unintended pregnancy, with consequences that present difficulties for the individual, family, and community.1 There are negative associations between early childbearing and numerous economic, social, and health outcomes.2–5 For society, unintended early childbearing has tremendous social and financial costs. 6 7 In response, communities have implemented various pregnancy prevention strategies for adolescents, several of which have been evaluated. Discrepant results of these evaluations have left the effectiveness of such strategies in doubt.
A recent meta-analysis found that school sex education programmes improved sexual knowledge.8 Several reviews have examined the effectiveness of pregnancy prevention programmes for adolescents in improving sexual behaviour. 2 9–14 All of these reviews included non-randomised observational studies; most did not include unpublished studies; and only one statistically combined study findings, although most of the studies were surveys.14
We undertook a systematic review that included non-published studies to avoid publication bias, 15 16 excluded non-randomised studies that tend to inflate treatment effects,17 and provided a summary measure to facilitate interpretation.
Methods
Eligibility criteria
We included published and unpublished randomised controlled trials of adolescents (ages 11 to 18 years) that evaluated pregnancy prevention programmes including sex education classes, school based clinics, family planning clinics, and community based programmes. We included studies that evaluated delay in initiation of sexual intercourse, consistent use of birth control, or avoidance of unintended pregnancy. All studies took place in North America, Australia, New Zealand, or Europe (excluding Eastern Europe) and were published in any language.
We excluded studies that evaluated prevention programmes offered in colleges or universities, those that evaluated interventions designed to prevent a second pregnancy, and those that evaluated only knowledge and attitudes. We also excluded studies that measured only condom use because study participants may have been using other methods of birth control and studies that measured only births because they omitted abortions.
Search for primary studies
Our literature search extended from 1970 to December 2000. We began with an extensive database we had established over the eight years of the McMaster Teen Project, a study that implemented and evaluated a sex education intervention.18 We searched the following computerised databases: CATLINE, CINAHL, conference papers index, dissertation abstracts online, Embase, ERIC, Medline, NTIS, POPLINE, PsycINFO, sociological abstracts, and the Cochrane controlled trials register. We reviewed the contents lists of the following journals from January 1993 to December 2000: American Journal of Public Health, Canadian Journal of Public Health, Adolescence, Health Education and Behavior, Family Planning Perspectives, Journal of School Health, Youth and Society (1993 only), Journal of Early Adolescence (1993 only), Journal of Adolescent Research (1993-4 only), and Journal of Adolescent Health Care (1993-6 only). We included dissertations, conference proceedings, technical reports, and other unpublished documents that met our inclusion criteria. We reviewed the reference lists of all papers for relevant citations. When all the relevant studies had been identified, we sent the list to experts to review for completeness. Twenty six randomised controlled trials described in 22 reports met our inclusion criteria.18–39
Quality assessment of studies
We assessed the methodological quality of the studies using a modified version of the rating tool developed by Jadad et al.40 We rated the studies according to appropriateness of randomisation, extent of bias in data collection, proportion of study participants followed to the last point of follow up (adequate follow up included data on ≥80% of the study participants at the last point of follow up), and similarity of attrition rates in the comparison groups (acceptable rates were within 2% of each other). We assigned 1 point for each (maximum of 4 points) and considered studies to be of poor quality if they scored ≤2.
Data extraction
In addition to data on quality assessment, two individuals independently extracted data on setting, participants, unit of randomisation and analysis, theoretical framework guiding the intervention, intervention, outcome variables, length of follow up, proportion followed to study completion, and study findings at the last follow up by sex (if possible).
For each study we established the number of participants in the intervention and control groups who had and had not experienced the event (for instance, initiation of sexual intercourse after intervention, consistent use of birth control, and pregnancy after intervention) for the last follow up period. To define consistent use of birth control we assessed use at every intercourse or use at last intercourse. Pregnancy rates included any measure that assessed whether a young woman had conceived or given birth or whether a young man had impregnated a young woman or fathered a child.
In all cases two individuals assessed the studies and extracted data, with discrepancies resolved by joint review and consensus. We reviewed assessment of methodological quality and data extraction with the 16 authors who provided additional information when necessary.
Data analysis
Ten of the 22 studies randomised clusters such as classrooms, schools, agencies, or neighbourhoods rather than individuals. Optimal analysis of cluster randomised studies involves adjustment that relies on the correlation within clusters. We could access these correlations from only one study18 and therefore used these data as estimates for the correlation in all such studies and for each outcome. This correlation value, along with the number and size of clusters in each of the nine other studies, provided a method for estimating the appropriate variance inflation and thus the extent to which studies using cluster randomisation would receive less weight than studies using individual randomisation.
For each study we calculated the odds ratio with 95% confidence intervals. We pooled odds ratios using the DerSimonian and Laird random effects model,41 tested for heterogeneity among studies using a χ2 procedure,42 and considered P<0.1 as an indication of heterogeneity. We performed analyses separately by sex, as sex differences may be missed when data are pooled.43
We tested 10 a priori hypotheses that might explain heterogeneity of study results: publication type (published and unpublished), control group intervention (alternate intervention and none), year of publication (before 1995 and 1995 or later), randomisation (appropriate and inappropriate), data collection (biased and unbiased), loss to follow up (≥80% and <80%), difference in loss to follow up between groups (≤2% and >2%), follow up period (≥12 months and <12 months), baseline differences (none, favouring control, and favouring intervention), and type of intervention (school based sex education, multifaceted programme, family planning clinic, and abstinence programme).
Results
Trial characteristics
Table 1 gives details of the 22 reports of 26 randomised controlled trials that met our eligibility criteria. Of the 22 reports, 17 were published, four were unpublished dissertations, and one was an unpublished report.
Description of studies that evaluated strategies to prevent unplanned pregnancies in adolescents*
Quality assessment of studies
Table 2 gives details of the assessment of quality. Only eight studies scored over 2 points of the possible 4. Only two studies scored the maximum 4 points. 28 36
Quality assessment of randomised controlled trials of interventions aimed at preventing pregnancy in adolescents*
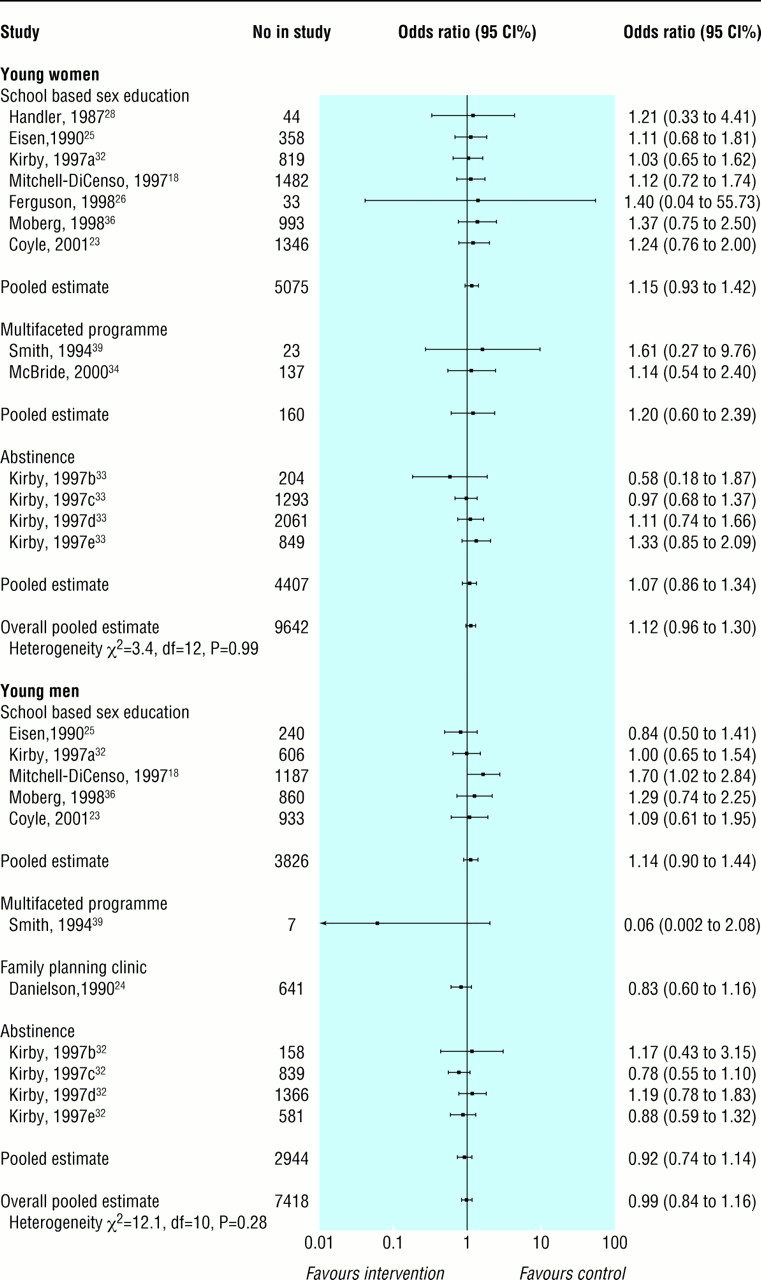
Initiation of sexual intercourse
Figure 1 shows the results of the meta-analysis on studies that looked at initiation of sexual intercourse. Thirteen studies in 9642 young women showed no delay in initiation of sexual intercourse (pooled odds ratio 1.12; 95% confidence interval 0.96 to 1.30). Results were consistent across studies (heterogeneity P=0.99). Results of 11 studies also showed no delay in initiation of sexual intercourse in 7418 young men (0.99; 0.84 to 1.16). There was no significant heterogeneity among the studies (P=0.28).

Effect of interventions on whether adolescents started to have sexual intercourse
{kind=link}
Use of birth control
Figure 2 shows the results for use of birth control at every intercourse. In 1967 eight studies of young women showed no improvement in use of birth control at every intercourse (0.95; 0.69 to 1.30). However, there was significant heterogeneity among studies (P=0.08) that was not explained by any of our 10 a priori hypotheses. Three studies of school based sex education in 1505 young men looked at whether they always used birth control. Results were remarkably consistent across studies (heterogeneity P=0.97) with a pooled estimate of 0.90 (0.70 to 1.16), indicating that the programmes did not improve use of birth control at every intercourse.

Effect of interventions on whether adolescents always used birth control
{kind=link}
Figure 3 shows results for use of birth control at last intercourse. Five studies of school based sex education programmes in 799 young women showed no improvement (1.05; 0.50 to 2.19), with significant heterogeneity (P=0.007) that was not explained by any of our 10 a priori hypotheses. Aarons et al found a large treatment effect in favour of the intervention (4.47; 1.60 to 12.51).19 However, there were substantial baseline differences in this study that favoured the treatment group: 39% of the young women in the intervention group used birth control the last time they had intercourse compared with only 27% in the control group. More young women in the control group lived in a single parent family (32% v 22%) and more participated in the free lunch programme (69% v 53%), indicating lower socioeconomic status. When the authors controlled for age, academic grades, and free lunch programmes (but not for the other baseline differences) the odds ratio was 3.86 (1.10 to 13.47). In addition, data collection in this study was anonymous, which prevented any matching of before and after questionnaire data.
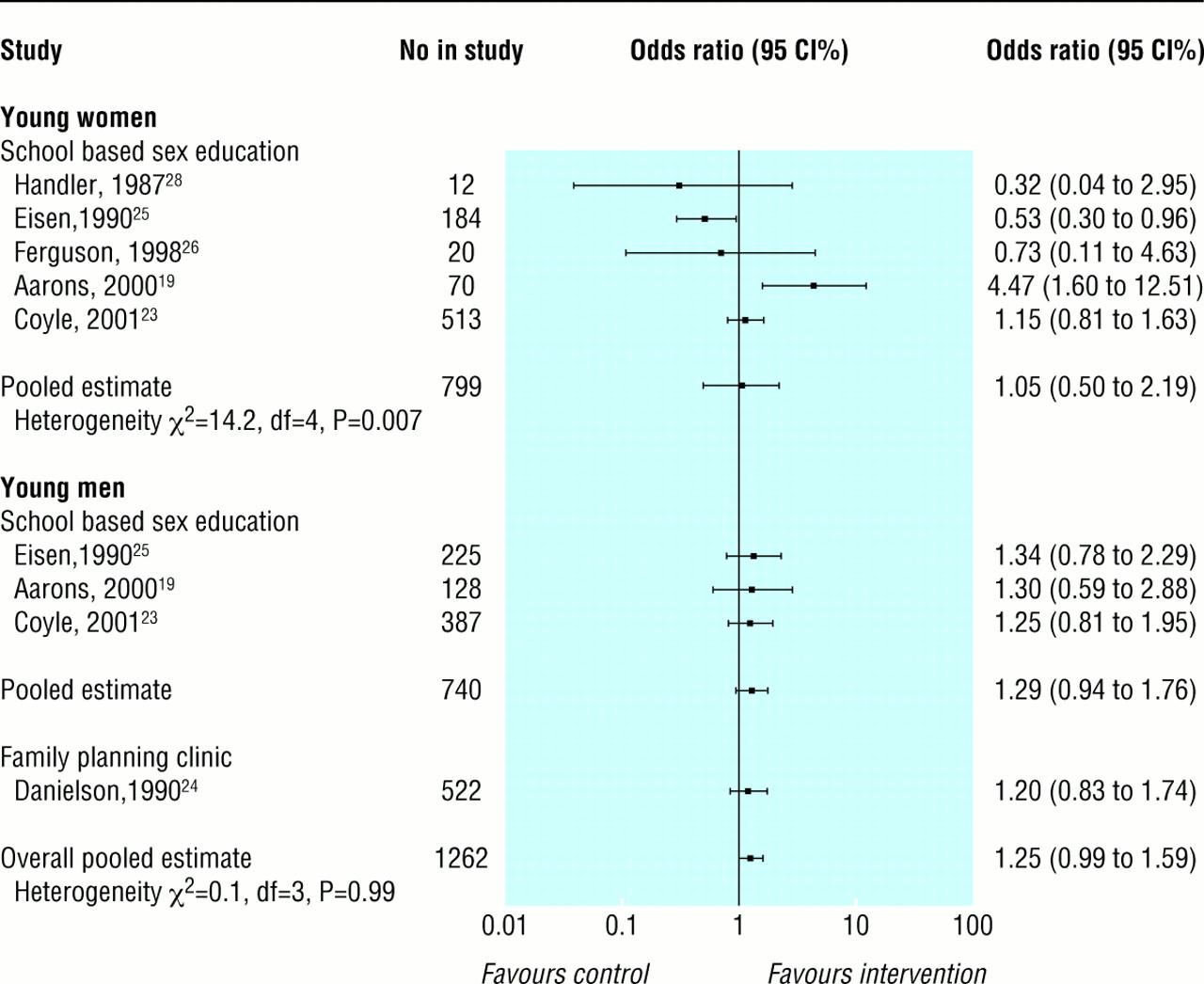
Effect of interventions on whether adolescents used birth control the last time they had sexual intercourse
{kind=link}
For use of birth control at last intercourse, four studies in 1262 young men had consistent results across studies (heterogeneity P=0.99), with a pooled estimate of 1.25 (0.99 to 1.59). The programmes therefore did not improve use of birth control by young men at last intercourse.
Pregnancy
Twelve studies in 8019 young women showed that the interventions did not reduce pregnancy rates (1.04; 0.78 to 1.40), and there was no significant heterogeneity among studies (P=0.23, fig 4). One study that evaluated a multifaceted programme did find a reduction (0.41; 0.20 to 0.83).20 At baseline, however, the control group had higher levels of previous course failure (P<0.04), school suspension (P<0.03), and teenage pregnancy (P<0.01). The authors excluded three of 25 sites where baseline differences were most problematic (these data were also excluded in our odds ratio calculation), adjusted for any remaining demographic differences, and still found a significant odds ratio of 0.41.

Effect of interventions on rates of pregnancy in adolescent women
{kind=link}
Figure 5 shows the effects of interventions on reducing pregnancies among the partners of 3759 young men. The pooled estimate of 1.54 (1.03 to 2.29) suggests that these interventions increased reported pregnancies. There was no significant heterogeneity among studies (P=0.58). Because Kirby et al did not report pregnancy data separately for young men and women we could not include their data in the meta-analyses. For the sexes combined they found no significant treatment effect (0.83, 0.34 to 2.01).32
Discussion
The results of our systematic review show that primary prevention strategies do not delay the initiation of sexual intercourse or improve use of birth control among young men and women. Meta-analyses showed no reduction in pregnancies among young women, but data from five studies, four of which evaluated abstinence programmes and one of which evaluated a school based sex education programme, show that interventions may increase pregnancies in partners of male participants.
Most of the participants in over half of the studies in our systematic review were African-American or Hispanic, thus over-representing lower socioeconomic groups. The interventions may be more successful in other populations. In all but five studies, participants in the control group received a conventional intervention rather than no intervention. It is possible that the control interventions had some effect on the outcomes and the tested interventions were not potent enough to exceed this effect. Finally, only eight of the 22 studies scored over 2 points out of the possible 4 points in the quality assessment. However, as poor methodological quality is more often associated with overestimates than underestimates of treatment effects it is unlikely that methodological weaknesses can explain the failure of the interventions to influence the outcomes measured.
Potential limitations
Although 10 of the 22 studies randomised clusters rather than individuals, we had data from only one of these studies18 to calculate correlations within clusters. We used these data as estimates for the correlation in all such studies to adjust for the cluster unit of randomisation. Secondly, despite testing 10 a priori hypotheses we were not able to explain the significant heterogeneity among studies that reported use of birth control in young women.
This review shows that we do not yet have a clear solution to the problem of high pregnancy rates among adolescents in countries such as the United States, the United Kingdom, and Canada.
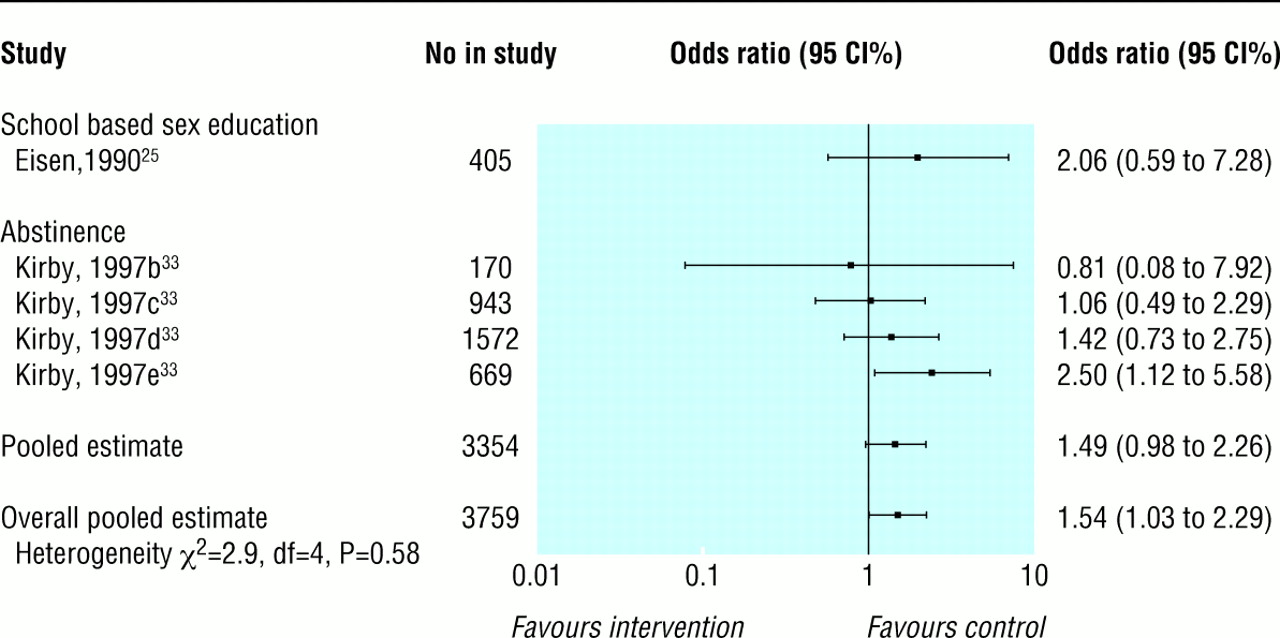
Effect of interventions on rates of pregnancy in partners of young men
{kind=link}
Direction of future research
There is some evidence that prevention programmes may need to begin much earlier than they do. In a recent systematic review of eight trials of day care for disadvantaged children under 5 years of age, long term follow up showed lower pregnancy rates among adolescents.44 We need to investigate the social determinants of unintended pregnancy in adolescents through large longitudinal studies beginning early in life and use the results of the multivariate analyses to guide the design of prevention interventions. We should carefully examine countries with low pregnancy rates among adolescents. For example, the Netherlands has one of the lowest rates in the world (8.1 per 1000 young women aged 15 to 19 years), and Ketting and Visser have published an analysis of associated factors.45 In contrast, the rates are 93 per 1000 in the United States,46 62.6 per 1000 in England and Wales,47 and 42.7 per 1000 in Canada.48 We should examine effective programmes designed to prevent other high risk behaviours in adolescents. For example, Botvin et al found that school based programmes to prevent drug abuse during junior high school (ages 12-14 years) resulted in important and durable reductions in use of tobacco, alcohol, and marijuana if they taught a combination of social resistance skills and general life skills, were properly implemented, and included at least two years of booster sessions.49
Few sexual health interventions are designed with input from adolescents. Adolescents have suggested that sex education should be more positive with less emphasis on anatomy and scare tactics; it should focus on negotiation skills in sexual relationships and communication; and details of sexual health clinics should be advertised in areas that adolescents frequent (for example, school toilets, shopping centres).50 None of the interventions in this review focused on strategies for improving the quality of sexual relationships. Sexual exploitation, lack of mutual respect, and discomfort in voicing sexual needs and desires are common problems in adulthood. Interventions to help adolescents learn about healthy sexual relationships need to be designed and evaluations of these interventions that follow the adolescents into adulthood should be done.
Acknowledgments
We thank Elena Goldblatt for developing the search strategy and conducting searches of the electronic databases; Janet Yamada, Nalagini Nadarajah, and Sheila McNair for performing hand searches of key journals, retrieving articles, and sending data to authors for verification; and Maureen Dobbins who reviewed studies for methodological quality. We also thank Doug Kirby for sharing his expert knowledge and experience in reviewing this literature, the 16 authors who verified data extraction and provided further detail about their studies, Brian Hutchison for his thoughtful suggestions, and Susan Marks for careful review of the final manuscript. ADiC is a member of the Cochrane Fertility Regulation Review Group.
Contributors: ADiC had the original idea for the systematic review, prepared the grant application for funding, determined keywords for searches, identified databases to search and journals to handsearch, reviewed the searches to identify potentially relevant papers, reviewed papers for relevance and study quality, extracted data, contacted authors to verify data and to identify any missed studies, and wrote the first draft of the manuscript. She is the guarantor of the study. GG assisted with the preparation of the grant application, reviewed searches for potentially relevant papers, reviewed papers for study quality, extracted data, assisted in developing the data analysis plan, and edited the manuscript. AW developed and supervised the data analysis plan and contributed to the paper. LG carried out the data analysis and contributed to the paper.
Footnotes
-
Funding National Health Research Development Program, Health Canada; Ontario Ministry of Health and Long-Term Care; Region of Hamilton-Wentworth Social and Public Health Services PHRED Program: A Teaching Health Unit affiliated with McMaster University and the University of Guelph. ADiC is a career scientist of the Ontario Ministry of Health and Long-Term Care
-
Competing interests None declared.