Reliability of N-terminal pro-brain natriuretic peptide assay in diagnosis of heart failure: cohort study in representative and high risk community populations
BMJ 2002; 324 doi: https://doi.org/10.1136/bmj.324.7352.1498 (Published 22 June 2002) Cite this as: BMJ 2002;324:1498
- F D R Hobbs (f.d.r.hobbs{at}bham.ac.uk), head of departmenta,
- R C Davis, clinical research fellowa,
- A K Roalfe, statisticiana,
- R Hare, research associatea,
- M K Davies, consultant cardiologistb,
- J E Kenkre, senior research fellowa
- a Department of Primary Care and General Practice, Primary Care Clinical Sciences Building, University of Birmingham, Birmingham B15 2TT
- b Department of Cardiology, Selly Oak Hospital, Birmingham B29 2PE
- Correspondence to: F D R Hobbs
- Accepted 4 April 2002
Abstract
Objective: To investigate the performance of a novel assay for N-terminal pro-brain natriuretic peptide (NT-proBNP) in diagnosing heart failure in various randomly selected general and high risk community populations.
Design: Community cohort study (substudy of the echocardiographic heart of England screening study).
Setting: Four randomly selected general practices in the West Midlands of England.
Participants: 591 randomly sampled patients over the age of 45, stratified for age and socioeconomic status and falling into four cohorts (general population, patients with an existing clinical label of heart failure, patients prescribed diuretics, and patients deemed at high risk of heart failure).
Main outcome measure: Sensitivity, specificity, positive and negative predictive values, likelihood ratios, and area under receiver operating characteristic curve for NT-proBNP assay in the diagnosis of heart failure.
Results: For NT-proBNP in the diagnosis of heart failure in the general population (population screen), a level of >36 pmol/l had a sensitivity of 100%, a specificity of 70%, a positive predictive value of 7%, a negative predictive value of 100%, and an area under the receiver operating characteristic curve of 0.92 (95% confidence interval 0.82 to 1.0). Similar negative predictive values were found for patients from the three other populations screened.
Conclusions: This NT-proBNP assay seems to have value in the diagnosis of heart failure in the community. High negative predictive values indicate that the assay's chief use would be to rule out heart failure in patients with suspected heart failure with normal concentrations of NT-proBNP. Positive results may identify patients who need cardiac imaging.
What is already known on this topic
Many primary care doctors rely on clinical diagnosis of heart failure, although the validity of such diagnosis is poor
Electrocardiography can be used to triage patients for echocardiography, but specialist interpretation may be needed
Assay of brain natriuretic peptide is a potential aid in the diagnosis of heart failure
What this study adds
Assay of N-terminal pro-brain natriuretic peptide (NT-proBNP) seems to be a reliable test for ruling out heart failure
Normal concentrations virtually exclude the diagnosis of heart failure, and very high levels effectively diagnose the condition; intermediate values require confirmation by echocardiography
Assay of NT-proBNP has potential as part of a diagnostic triage in patients presenting with symptoms suggestive of heart failure or in screening populations at high risk
Introduction
Heart failure is an increasingly common disorder,1 with a prevalence of around 2% in developed countries.2 It is characterised by very poor prognosis and quality of life for patients, 3 4 and is responsible for very high healthcare costs. As outcomes in heart failure are linked to the stage of disease, early and accurate diagnosis is needed to guide appropriate treatment strategies. Despite the need for accurate diagnosis many doctors, especially in primary care, rely on diagnosing heart failure on clinical grounds alone.5
Clinical diagnosis of heart failure is not possible on the basis of European and American guidelines, 6 7 as objective evidence of cardiac dysfunction is needed, along with the presence of appropriate symptoms, before a diagnosis is confirmed. Improving the reliability of diagnosis is essential, as determining the aetiology and stage of heart failure leads to different management choices, such as angiotensin converting enzyme inhibitors and β blockers in most patients with left ventricular systolic dysfunction, 8 9 spironolactone in patients with severe heart failure,10 or surgery if appreciable valve disease exists. These treatments improve symptoms, quality of life, and prognosis of disease and reduce healthcare utilisation and costs.
The need for effective diagnostic and treatment strategies in heart failure is immense: the condition occurs in at least 2.3% of the adult population aged over 45, rising to 4% in over 75 year olds.2 Symptomatic heart failure has a major impact on patients and healthcare systems: its prognosis is worse than those of breast cancer or prostate cancer, and its treatment costs are second only to those for stroke, mainly owing to high admission rates.11 Furthermore, diagnosis needs to be made early, when there may be no symptoms, as treatment can delay or reverse progression of disease.12 Diagnostic methods may therefore need to encompass screening strategies, 13 14 as well as identification of patients with symptoms.
The investigation most commonly used to confirm the diagnosis of heart failure is echocardiography, which offers a detailed, semiobjective assessment of ventricular and valve function. However, access to echocardiography is limited in many healthcare systems,5 especially for primary care physicians, who see most potential cases. Not surprisingly, the validity of a clinical diagnosis of heart failure in primary care is poor, with high rates of misdiagnosis when patients are assessed against objective criteria, ranging from 25% to 50% accuracy. 15 16
Do alternative methods exist for diagnosing heart failure or enabling appropriate triage of patients for echocardiography? One option is electrocardiography, as a normal recording will, in most cases, exclude left ventricular dysfunction.17 However, changes on the electrocardiogram may be subtle, and primary care physicians18 (and hospital doctors19) are unreliable in assessing such changes. Interpretation of electrocardiograms may, therefore, still need referral to a cardiologist for a specialist opinion.20 Chest radiography is another option, but no data are available on its reliability in diagnosing heart failure.15
One potential diagnostic aid is the assessment of patients by assay of brain natriuretic peptide. Brain natriuretic peptide is a biologically active peptide of 32 amino acids, with vasodilator and natriuretic properties, which is cleaved from the 108 amino acid pro-brain natriuretic peptide released from the cardiac ventricles in response to stretching of the chamber. The second remnant after cleavage, N-terminal pro-brain natriuretic peptide (NT-proBNP), is a 76 amino acid peptide with no known biological function, which circulates at higher concentrations than brain natriuretic peptide and may represent cardiac status over longer periods. Studies of brain natriuretic peptide to date have been small, and data in different subgroups of patients are conflicting. 21 22 No reliable data exist on the performance of assays for brain natriuretic peptide assays in the diagnosis of heart failure in the general population. NT-proBNP has been even less investigated.16 This study provides original data on the utility of a novel NT-proBNP assay in the diagnosis of heart failure.
Methods
This is a prospective substudy of the echocardiographic heart of England screening (ECHOES) study of the prevalence of left ventricular dysfunction and heart failure.2 The main study was carried out in 16 randomly selected primary care practice populations in England after stratification for age and socioeconomic status. Patients were randomly selected from each of four population cohorts, identified in each practice from computerised practice registers: randomly sampled patients from those aged 45 years and older (general population screen); patients with a clinical diagnostic label of heart failure; patients prescribed diuretic drugs; and patients at high risk of heart failure (history of myocardial infarction, angina, hypertension, or diabetes).
We conducted this substudy in the last four practices, containing the final 607 consecutively screened patients randomly selected from the four target groups (307 in the general population, 103 with an existing clinical diagnosis of heart failure, 87 taking diuretics, and 134 at high risk of heart failure, with some sampled from more than one cohort). These practices were representative of the socioeconomic spread of patients achieved by the initial stratification. All patients gave informed consent, and the study had full ethical approval.
We screened patients by history, New York Heart Association functional class, clinical examination, quality of life (SF-36 health status questionnaire), spirometry, resting 12 lead electrocardiography, and echocardiography, including Doppler studies. We diagnosed heart failure on the basis of the agreed gold standard of the European and American guideline criteria (box). Three experienced cardiovascular clinicians conducted blinded adjudication of clinical records in equivocal cases. Aetiologies for heart failure included left ventricular systolic dysfunction, atrial fibrillation, and significant valve disease. We made no attempt to define diastolic heart failure in this study.
European Society of Cardiology criteria for diagnosis of heart failure
To satisfy the diagnosis of heart failure, there must be:
Appropriate symptoms of heart failure
Objective evidence of cardiac dysfunction on echocardiography and electrocardiography
Appropriate response to relevant treatment, in cases of doubt
Echocardiography is the most practical tool to demonstrate cardiac dysfunction
A research fellow took blood for the peptide assay from the right antecubital fossa of consenting patients after five minutes' supine rest, into 5 ml K+EDTA tubes. Blood was kept at room temperature for up to 24 hours before transport to a local laboratory for centrifugation and freezing of plasma to −20°C. Once a week the frozen samples were collected for central storage at −70°C. Assays of NT-proBNP (Roche Diagnostics, Germany) were subsequently performed at a central independent laboratory, blinded to the results of the screening assessments. The NT-proBNP immunoassay—an enzyme linked immunosorbant assay (ELISA)—required only three operator dependent steps and total incubation of under two hours.
Analysis
We assessed the diagnostic performance of the assay by using receiver operating characteristic curves, formed by plotting sensitivity on the y axis and 1−specificity on the x axis for all possible cut-off values of each diagnostic test. The overall discriminatory ability of each test is shown by the area under the curve.
In addition to the area under the curve, we identified the cut-off value from the general population that maximised sensitivity without much loss of specificity. Such an analysis maximises the negative predictive value of a test, which is an appropriate aim for a test performed in primary care on symptomatic patients. We also calculated likelihood ratios as a measure of the extent to which the pre-test odds are altered by the test results (values >1 increase the odds; values <1 decrease the odds). We then applied the cut-off values to the other groups. We present the resulting positive and negative predictive values and likelihood ratios, with confidence intervals.
We used multiple logistic regression analysis to determine whether the peptide assay gave improved diagnosis of heart failure over the known clinical predictors of sex, electrocardiogram abnormality, and history of myocardial infarction or diabetes. Concentrations of NT-proBNP were not normally distributed and were log transformed before analysis. We compared the resultant models by using log likelihood χ2 tests. We used SPSS and Microsoft Excel for statistical analyses.
Results
Five hundred and ninety one (97%) of 607 eligible patients consented to supply a blood sample. Table 1 lists the basic demographics of the population screened, and table 2 gives the overall performance characteristics of the assay.
Characteristics of patients (n=591)
Area under receiver operating characteristic curve, sensitivity, specificity, predictive values, and likelihood ratios for NT-proBNP, with a cut-off value of 36 pmol/l, in the diagnosis of definite heart failure. Values in parentheses are 95% confidence intervals
The assay detected definite heart failure in a total of 52 people from the four diagnostic groups—seven from the random general population, 35 from the patients with an existing diagnosis of heart failure, 14 from patients on diuretic treatment, and nine in the high risk group (13 patients were in more than one group). The most frequent causes of heart failure were left ventricular systolic dysfunction, atrial fibrillation, and significant valve disease, or combinations of the three.
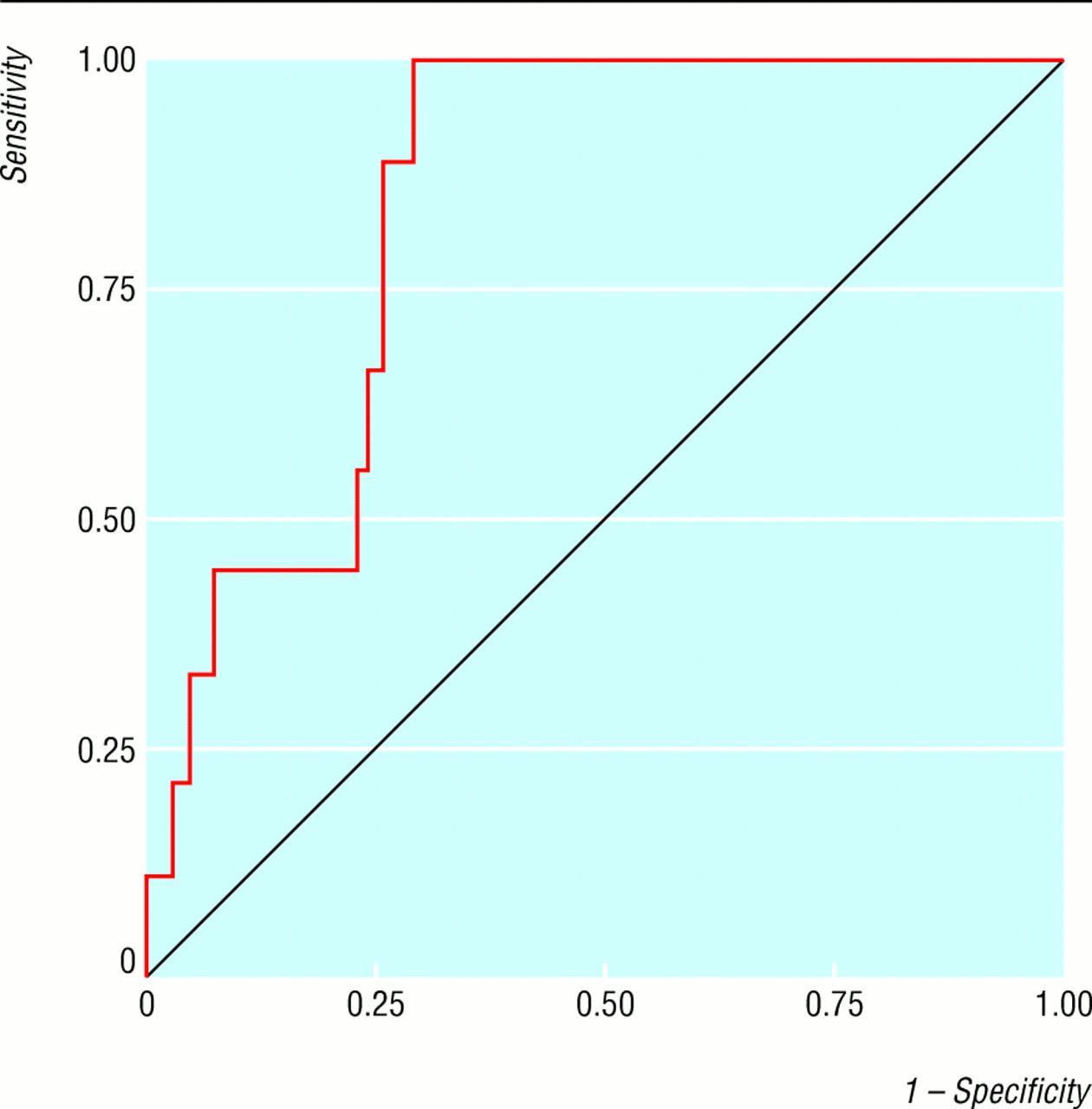
In the general population sample, an NT-proBNP concentration of >36 pmol/l had a sensitivity of 100%, a specificity of 70%, a positive predictive value of 7%, and a negative predictive value of 100%. The likelihood ratio of a positive test result was 3.37, and the likelihood ratio of a negative result was 0 (table 2). The area under the receiver operating characteristic curve was 0.92 (95% confidence interval 0.82 to 1.00) (fig 1).

Receiver operating characteristic curves for NT-proBNP in the diagnosis of definite heart failure in the general population
{kind=link}
Similar performance characteristics for diagnosis of heart failure were found when we used the same cut-off values in the other three screened population cohorts (figs 2, 3, and 4). Negative predictive values ranged from 97% to 100%, and likelihood ratios of a negative result ranged from 0 to 0.18 (table 2).

Receiver operating characteristic curves for NT-proBNP in the diagnosis of definite heart failure in the population with an existing clinical (not validated) diagnosis of heart failure made in primary care
{kind=link}

Receiver operating characteristic curves for NT-proBNP in the diagnosis of definite heart failure in the population taking prescribed diuretics
{kind=link}
Receiver operating characteristic curves for NT-proBNP in the diagnosis of definite heart failure in the high risk population
{kind=link}
Logistic regression models predicting definite heart failure, with explanatory variables of sex, history of myocardial infarction or diabetes, and Q waves or bundle branch block pattern on electrocardiogram, were significantly improved with the addition of log NT-proBNP (χ2=62.0, 1 df, P<0.001).
Discussion
Although several studies on assays for brain natriuretic peptide in select patient groups have been published, these are the first data on the performance characteristics of an assay for NT-proBNP in a large generalisable series of randomly selected adults with validated diagnoses of heart failure and with a comparator normative population randomly selected from the same populations as the cases. The assay was also used under the same conditions and constraints as occur in routine clinical practice.
We avoided spectrum bias in this analysis by presenting the performance characteristics in the four screened populations separately. The reduced numbers limit the precision of the estimates, but the negative predictive values and likelihood ratios of a negative result are very similar across the four populations. Other common confounders of diagnostic studies—namely, verification bias, treatment paradox, and reference standard error—were minimised. In the case of treatment paradox, any influence of drug treatment would have been to reduce the concentrations of natriuretic peptide and thus lead to underestimation of the true test performance.
We have shown NT-proBNP assays to be of value in diagnosing heart failure within a representative community based general adult population and also within at risk populations. The area under the receiver operating characteristic curves for NT-proBNP in the diagnosis of definite heart failure in the general population (0.92) contrasts with the area under the curve for cervical cytology of 0.723 and that for breast mammography of 0.85.24
Importantly, we have shown that the natriuretic peptide assay retains its utility despite samples being handled as they would be in the everyday practice of primary care—that is, collection by practising nurses and storage at room temperature for some hours before transfer to laboratory settings or freezing at domestic freezer temperatures. Previous studies have mostly used specialised in-hospital handling of samples, including immediate chilled centrifugation and rapid freezing of samples to −70°C.
Another important finding is that NT-proBNP levels are elevated in all major causes of heart failure—left ventricular systolic dysfunction, atrial fibrillation, and valve disease. However, we provide no data on the utility of the assay in diagnosing diastolic heart failure.
The very high negative predictive values, and corresponding low likelihood ratios of a negative result, of the assay make heart failure very unlikely with concentrations below the cut-off value, suggesting that the most appropriate use of the assay in routine practice would be as a rule out or exclusion test. The low likelihood ratios of a negative result are comparable to those for colposcopy, which range from 0.002 to 0.38.25 Elevated concentrations of NT-proBNP should therefore trigger further cardiac investigation, including echocardiography. If left ventricular systolic dysfunction is excluded, elevated concentrations of NT-proBNP may indicate other problems, such as diastolic dysfunction,26 left ventricular hypertrophy, unstable angina, or pulmonary hypertension.27
The main limitation of the study relates to it being based on a major epidemiological study. The findings are reliable for assay performance in a general population screen of people aged over 45 and for screening in the three other target populations of the ECHOES study, although the individual population numbers become small. However, general population screening is not likely to be a realistic proposal, despite the prevalence and prognosis of heart failure. These data suggest that, in clinical practice, the assay would have three practical uses: screening patients with existing clinical labels of heart failure (70 of the 103 patients so categorised in this study had heart failure ruled out on NT-proBNP testing); triaging patients presenting with symptoms suggestive of heart failure (shortness of breath, lethargy) for echocardiography; and screening patients at high risk of heart failure. We suspect the assay would perform well in these settings, but the first indication was not formally tested in this study, and the third indication was tested in only 134 patients. These data are sufficiently positive to justify formal trials of the assays in real life strategies for screening symptomatic patients and those at high risk.
Acknowledgments
Contributors: FDRH and MKD were joint principal investigators and grant holders on the main study, with FDRH as grant holder of this substudy. FDRH led the design and execution of the study and analysis. RCD conducted most of the clinical assessments and reporting and made a major contribution to analysis. JEK and RH contributed to study design and analysis and overall study management. AKR did the statistical analysis. All authors contributed to drafts of the paper. FDRH is the guarantor.
Footnotes
-
Funding The ECHOES study was funded by the NHS R&D cardiovascular disease and stroke programme. The costs of collecting and handling the samples were supported by an NHS Regional R&D grant, and the assays and technical support were donated by J Trawinski and J Baumann of Roche Diagnostic Solutions.
-
Competing interests FDRH is a member of the European Society of Cardiology (ESC) Working Party on Heart Failure, chair of the British Primary Care Cardiovascular Society, and Treasurer of the British Society for Heart Failure. MKD is chairman of the British Society for Heart Failure. FDRH and MKD have received travel sponsorship and honorariums from several biotechnology and pharmaceutical companies with cardiovascular products for plenary talks and attendance at major cardiology scientific congresses and conferences.