Paediatric cardiac surgical mortality in England after Bristol: descriptive analysis of hospital episode statistics 1991-2002
BMJ 2004; 329 doi: https://doi.org/10.1136/bmj.329.7470.825 (Published 07 October 2004) Cite this as: BMJ 2004;329:825
- Paul Aylin (p.aylin{at}imperial.ac.uk), clinical senior lecturer1,
- Alex Bottle, researcher1,
- Brian Jarman, emeritus professor1,
- Paul Elliott, professor of epidemiology and public health, faculty of medicine1
- 1 Dr Foster Unit at Imperial College London, Department of Epidemiology and Public Health, Imperial College School of Medicine, London W2 1PG
- Correspondence to: P Aylin
- Accepted 4 August 2004
Abstract
Objective To describe trends in mortality of open cardiac surgery in children in Bristol and England since 1991.
Design Retrospective analysis of hospital episode statistics data.
Setting All open cardiac surgery of children in England.
Population Patients younger than 16 undergoing open cardiac surgical procedures in England between April 1991 and March 2002. Three time periods were defined: epoch 3 (April 1991 to March 1995), epoch 5 (April 1996 to March 1999), epoch 6 (April 1999 to March 2002).
Main outcome measure Mortality in hospital within 30 days of a cardiac procedure.
Results We identified 5221 open operations between April 1996 and March 2002 in children under 1 year and 6385 in children aged 1-15 years. Mortality for all centres combined fell from 12% in epoch 3 to 4% in epoch 6. Mortality in children under 1 year at Bristol fell from 29% (95% confidence interval 21% to 37%) in epoch 3 to 3% (1% to 6%) in epoch 6, below the national average. The reduction in mortality did not seem to be due to fewer high risk procedures or an increase in the numbers of low risk cases. Oxford had a significantly higher mortality than the national average in all three epochs (11% (5% to 18%) in epoch 6), which was not affected by adjusting for procedure or the inclusion of cases with missing outcomes.
Conclusions At Bristol, mortality for open operations in children aged under 1 year has fallen markedly, to below the national average. Nationwide mortality has also fallen. Improved quality of care may account for the drop in mortality, through new technologies or improved perioperative and postoperative care, or both.
Introduction
One of the key issues for the Bristol inquiry1 was whether mortality statistics in Bristol were unusual compared with other specialist centres. Work commissioned by the inquiry examined hospital episode statistics data on cardiac surgery carried out in children at Bristol and other major centres in England.2 The main finding was that mortality in Bristol was about twice as high as in other centres from April 1991 to March 1995, for open operations in children aged under 1 year.
We report data on the performance of Bristol Royal Infirmary and that of the other major centres in England since the original research.
Methods
We obtained hospital episode statistics (April 1991-March 2002) for open cardiac surgical procedures in children in England, including the 11 major centres. The two age groups we defined were children aged under 1 year and children aged between 1 and 15. We used the same selection criteria, the same broad class of open procedures (requiring cardiopulmonary bypass), and the 11 procedure groups defined in an earlier report3 to compare mortality in hospital within 30 days of a surgical procedure for each centre with the overall mortality for all centres combined. Several steps were required to link finished consultant episodes (the time spent under the continuous care of a specific consultant) within a hospital admission to determine the final outcome on discharge. Where this could not be done (because of fields with missing data), we could not determine the outcome.
In the original research, four “epochs” were defined, and data for the third and fourth were available in hospital episode statistics4: epoch 3 comprised April 1991 to March 1995, and epoch 4, April 1995 to December 1995. We focus on epoch 3; epoch 4 was a short period containing few operations, as the two previous surgeons at Bristol had essentially ceased complex cardiac surgery on children. For comparison, we defined two further epochs: epoch 5 from April 1996 to March 1999; and epoch 6 from April 1999 to March 2002. We calculated mortality (including exact binomial confidence intervals) for each centre for each epoch. We used Bayesian simulation methods5 to calculate the probability that each centre is ranked worst.
We used binary logistic regression for mortality to calculate odds ratios relative to the overall mean. We used the 11 open procedure groups defined previously to adjust for procedure.3 To test the robustness of these analyses to data quality issues, we calculated the odds ratios, including all spells with a missing outcome, by coding them as discharged alive. We also looked at data by year.
Results
In epoch 3, we identified 3509 open cardiac operations in England in children under 1 year for the original study and 4741 such operations in children between 1 year and 15 years; we identified a further 5221 and 6385 operations, respectively, between April 1996 and March 2002. For epoch 3, 5.4% (190 cases) of open operations in children aged under 1 year were carried out in hospitals other than the 11 specialist centres. In epoch 6, this figure declined to 0.2% (five cases).
For children aged 1 to 15, Harefield had a significantly raised mortality in the original analysis (12%, 95% confidence interval 8% to 16%, P < 0.001) in epoch 3, but it has since merged with the Brompton Hospital and their results are combined for consistency over time. However, even their combined mortality remained significantly high (8%, 6% to 10%, P < 0.001) compared with all centres combined in epoch 3. For epoch 5 and 6, Harefield-Brompton were not significantly high. No other centre in epochs 3, 5, or 6 had a significantly raised mortality. The national mortality in this age group also decreased from 5% in epoch 3 to less than 2% in epoch 6.
Figure 1 shows mortality for open operations for children under 1 year in three epochs for the 11 specialist centres in descending order, by total volume of cases. It shows Bristol with a mortality of 29% (21% to 37%, P < 0.001) in epoch 3, but mortality falls to 5% (2% to 9%, P = 0.798) in epoch 5 and 3% (1% to 6%, P = 0.801) in epoch 6. Mortality for all centres combined declined from 12% in epoch 3 to 7% in epoch 5 and 4% in epoch 6. Oxford had a significantly higher mortality than the national average in all three epochs: 19% (12% to 27%, P = 0.010) in epoch 3, 14% (8% to 22%, P = 0.003) in epoch 5, 11% (5% to 18%, P = 0.001) in epoch 6. If Bristol is excluded from the first epoch, Oxford had the highest mortality for all three epochs. However, it too had a downward trend in mortality. The probability of at least one centre having a significantly high mortality in all three epochs by chance alone is less than 0.0002. The probability that Oxford had the highest mortality in epoch 3 was 3% (if Bristol is excluded it was 72%), 48% in epoch 5, and 79% in epoch 6 (see table A on bmj.com).
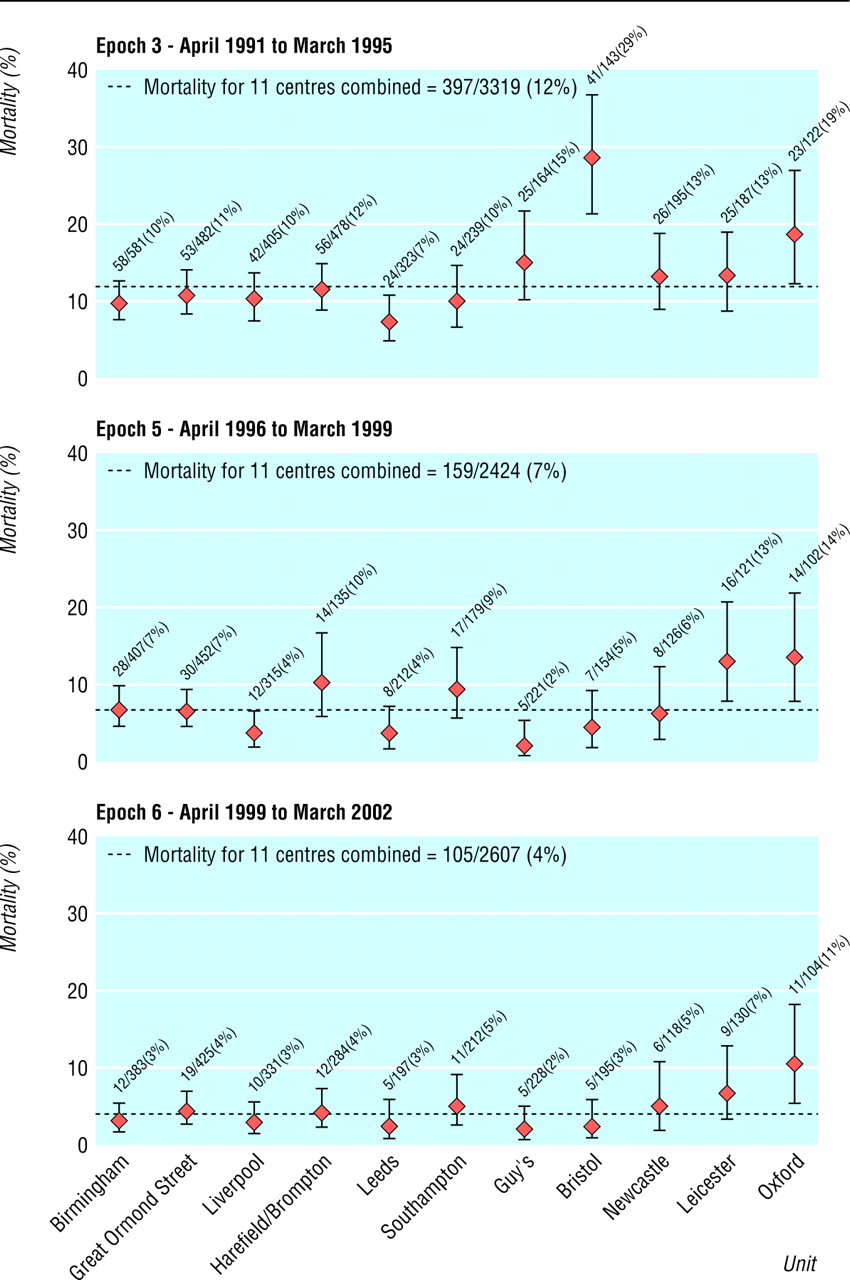
Mortality from open procedures in children aged under 1 year for 11 centres in three epochs; data derived from hospital episode statistics. Centres are listed by descending volumes of cases
{kind=link}
Adjustment for procedure by using the 11 open procedure groups made little difference to the pattern of mortality. Oxford remained as the only centre with a significantly high mortality over all three epochs examined, with an odds ratio of 1.75 (1.16 to 2.62, P = 0.007) in epoch 3, 2.11 (1.13 to 3.95, P = 0.019) in epoch 5, and 4.14 (2.12 to 8.09, p < 0.001) in epoch 6, compared with the overall mean of the centres combined (see table B on bmj.com). The only other centres that had a significantly high odds ratio after adjustment for procedure were Harefield-Brompton (odds ratio 2.04, 95 confidence interval 1.14 to 3.65, P = 0.016) in epoch 5 and Leicester (3.24, 1.88 to 3.95, P < 0.001) also in epoch 5 (see figure A on bmj.com).
The proportion of admissions with outcomes unknown improved over time from 5.1% in epoch 3 to 1.4% in epoch 6. However, the proportion varied between centres. For example, in 1995-6, 75% of outcomes in Leicester were unknown, and during epoch 5, 46% of outcomes in Harefield-Brompton were unknown. In Bristol, the proportions unknown fell from 17% in epoch 3 to 1% in epoch 6. Oxford's percentage of operations with an unknown outcome was low (maximum of 1.9% in any of the three epochs examined). We carried out a sensitivity analysis to examine the effect of including admissions with a missing outcome, recoded as discharged alive (figure B on bmj.com). Oxford remained the only centre with a significantly high mortality in all three epochs, with an odds ratio of 1.80 (1.20 to 2.70, P = 0.004) in epoch 3, 2.25 (1.20 to 4.19, P = 0.011) in epoch 5, and 4.17 (2.14 to 8.13, P < 0.001) in epoch 6. The odds ratio for Harefield-Brompton dropped in epoch 5 to 1.03 (0.58 to 1.81, P = 0.928), indicating that their high mortality in this epoch may have been due to incomplete data.
Figure 2 shows annual mortality for Bristol and for all centres combined, together with total numbers of open operations in children under 1 year. Within all 11 centres, the total number of open operations per year for children under 1 year varied between 732 in 1991-2 and 967 in 1996-7, with no obvious trend; for older children aged between 1 and 15, numbers of operations fell by 11.8% from an average of 1185 per year in epoch 3 to 1045 in epoch 6 (not shown). In epoch 3, Bristol was carrying out an average of around 43 open operations per year on children under 1. This has now increased to 66 patients a year in epoch 6.

Mortality (based on admissions with known outcome) for and number of open operations on children aged under 1 year from April 1991 to April 2002 in 11 English centres; data derived from hospital episode statistics
{kind=link}
For Bristol, mortality declined rapidly from 1995. For all centres combined, mortality also fell, but this seems to be a continuous trend throughout the entire period, which is significant (P < 0.01). The small peak in 1995 coincided with some missing data on outcomes, particularly at Leicester, in that year; if missing outcomes are reclassified as “alive when discharged,” the peak disappears.
The table shows a comparison of death rates, average annual numbers of procedures, and percentage changes from epoch 3 to epoch 6 for the 11 procedure groups. All show a marked reduction in mortality (between 36% and 91%). The number of Fontan-type operations nearly doubled (94% increase), and their mortality fell from 18% to 1.6%. The number of procedures to correct tetralogy of Fallot (16%) and closure of ventricular septal defect (13%) also rose. Numbers of procedures for total anomalous pulmonary venous drainage and mitral valve procedures remained about the same. Numbers fell for all other procedures listed, ranging from −38% for procedures to correct interatrial transposition of the great arteries to −14% for repair of atrial ventricular septal defects. When we adjusted for procedure for all units combined, mortality was still markedly higher in epoch 3 than in epoch 6, with an odds ratio of 3.5 (2.8 to 4.6).
Comparison of mortality (based on admissions with known outcomes), average annual numbers of procedures, and percentage changes from epoch 3 to epoch 6 for 11 defined procedure groups in all centres in England; data derived from hospital episode statistics
Discussion
At Bristol, since the events that led to the inquiry1 and after considerable changes in the paediatric cardiac surgery service were introduced from 1995 onwards, mortality for open operations in children aged under 1 has fallen markedly, so that it is no longer an outlier. The national trend is towards a lower mortality, as reflected in the Society of Cardiothoracic Surgeons of Great Britain and Ireland's own published figures.6 Several factors might have contributed to the national reduction in mortality: chance, data quality, a reduction in the number of high risk cases or increase in the number of low risk cases operated on, or improved quality of care.
Data quality
Data quality is an important issue, although extensive comparisons with other data sources for the original research showed that hospital episode statistics data were of sufficient quality to be used for the analysis.2 4 A recent paper also showed that hospital episode statistics are suitable to be used to monitor deaths in hospital routinely.7 Missing data on outcomes could, however, bias results. We examined the sensitivity of our analyses to include admissions where the outcome is unknown, and it makes little difference to the overall pattern of mortality. The same centres have a significantly high mortality in epoch 3 (Bristol and Oxford), epoch 5 (Oxford and Leicester), and epoch 6 (Oxford), even after adjustment for procedure. Our evidence also shows that the quality of data, at least in terms of completeness, is improving.
Possible change in procedures or cases
A reduction in the number of high risk procedures or cases, or an increase in low risk ones, might reduce mortality; but no indication exists that any such systematic shifts have occurred. The numbers of procedures that are now carried out have changed: the reduction in repair of complete atrial ventricular septal defect may be due to increased antenatal diagnosis (with termination of pregnancy) of babies with Down's syndrome8; the reductions in secundum atrial septal defect procedures are probably due to the increasing number of patients undergoing percutaneous device closure by cardiologists; the reduction in truncus arteriosus may again be because of antenatal diagnosis and termination; cardiologists now carry out most pulmonary valve procedures by percutaneous intervention, and many of the children who would have had aortic valve replacements in the past are now having Ross procedures.9 We are not aware of any major changes in specific surgical technique except for the Nor-wood procedure for hypoplastic left heart syndrome, with a change in positioning of the shunt to provide pulmonary blood flow. This may also account for the increase in the number of Fontan operations, as all these children go on to have the procedure as the third stage. Adjustment for procedure between epochs still shows a marked reduction in mortality over time.
Open procedures in England have shifted towards being carried out exclusively by the 11 specialist centres; currently, practically no such procedures in children under 1 year are carried out outside these centres. Improvements in intensive care may also have contributed to the improvement in mortality, with an increasing number of appointments of dedicated intensivists, the introduction of more effective treatment of high pulmonary vascular resistance,10 and improved techniques of post operative mechanical ventilation.
Reasons for Oxford's death rates
Oxford alone had a significantly raised mortality in epoch 6. Although this was based on only 11 deaths, Oxford had a consistently raised mortality for all three epochs examined. It must be recognised, however, that in looking at 11 centres over three epochs, an element of multiple comparisons has to be considered. The consistency of Oxford's high mortality relative to other units over all three epochs makes this less of an issue, with a probability of this happening by chance alone of less than 0.0002. Even after adjustment for procedure and the inclusion in the analysis of all admissions with unknown outcomes recoded as alive, Oxford remains the only centre with significantly raised mortality for all three epochs. There may be differences in case mix that we have been unable to adjust for. We were not able, within hospital episode statistics, to examine and adjust for risk factors such as underlying heart function, lung function, kidney function, and other vascular conditions. Some concern has been expressed over cardiac surgery at Oxford in the past.11 The unit became aware in 1999-2000 of a possible downturn in their results with respect to transpositions of the great arteries and stopped carrying out these from May 2000. The unit's own more recent data indicate that mortality has fallen since then (J Morris, medical director, Oxford Radcliffe Hospitals NHS Trust, personal communication, 2 April 2004).
What is already known on this topic
The Bristol inquiry between 1991 and 1995 showed that Bristol had a much higher mortality for open operations in children aged under 1 year than other major centres
What this study adds
Recent hospital episode statistics data show that in Bristol mortality has fallen markedly after the changes there
Nationally, a gradual fall in mortality has become evident from the time data were first available
The Oxford Radcliffe Hospitals NHS Trust contributes to the central cardiac audit database,12 which collects more detailed information on case mix. An independent review of NHS paediatric and congenital cardiac services concluded that surgical results for all centres, based on only one year of data from the central cardiac audit database, all fall within a very narrow range and compare favourably with international results.13 A recent paper, again based on the database,14 found no detectable difference in 30 day or one year survival between any of the 13 UK tertiary centres for congenital heart disease; however, the analysis considered only one year of data (limiting statistical power), the centre comparisons were based on only six procedures, and no attempt was made to adjust for case mix. A reanalysis of our data for single years from 1991-2 to 1994-5 by using the same criteria indicates that the high mortality at Bristol would probably have been missed, reaching only borderline significance in one year, 1993-4 (11.7%, 99% confidence interval 4.7% to 22.7%) compared with a national average of 4.7% (99% confidence interval 3.3% to 6.3%).
Conclusion
Mortality at the Bristol Royal Infirmary has fallen markedly after the changes there, and a more gradual reduction in national mortality is evident from the time these data were first available. Improved quality of care may account for the decrease in mortality, through new technologies or improved perioperative and post-operative care, or both. Whatever the reasons for the reduction in mortality, this seems to be good news for patients and parents.
Footnotes
-
 Additional figures and tables are on bmj.com
Additional figures and tables are on bmj.comWe thank Leslie Hamilton (consultant cardiac surgeon, Freeman Hospital, Newcastle upon Tyne) for his helpful comments on our draft and particularly for his advice on changing patterns of surgical and post-operative practice. We also thank Nicky Best (reader in statistics, Imperial College London) for her advice on statistical matters.
-
Contributors PA and PE were involved in the original research. PA and BJ devised this follow up work. PA and AB carried out the data extract and analyses. PA and PE drafted the paper. All investigators contributed comments on drafts.
-
Competing interests The work was funded by Dr Foster Limited. BJ served on the panel for the Bristol Royal Infirmary inquiry. PA was an expert witness for the inquiry. PE was on the statistical review panel for the inquiry.